News & Articles
Reaching the Hardest to Reach: Public Health and the Digital Divide
Color

Public Health and the Digital Divide
The United States is reckoning with a truth it can’t ignore: entrenched health inequities exist in every city, county, and state. Too often, the shade of our skin, the size of our bank account, or the zip code on our mail is a powerful predictor of our life expectancy. Access to housing, jobs, education, and social support is a necessary foundation for a long, healthy life. Yet, underneath all of these basic human needs is access to information, which is itself unequally distributed across the country.
Public Health — the field responsible for ensuring health across the population — serves as the north star of health equity. At Color, we know that if we want to close the gaps in access to health, we need to develop new ways of reaching the hardest-to-reach. “Health equity” means that those who need the most help get the most help. Digital tools present a promising opportunity for bridging the divide in health, but digital tools are only as good as the supporting infrastructure. A closer look at digital equity across the country reminds us that, in some communities, horse ownership is more likely than computer ownership.
Health departments often cover vast geographic areas. 70% of health departments in the US operate at the county level. This means that a single department is potentially responsible for millions of lives across thousands of square miles. Take, for example, Kern County, California. Covering an expanse of 8,163 square miles (roughly the size of the entire state of New Jersey), the Kern County Health Department is responsible for protecting the lives of nearly one million residents. They must do this on an average of $138 per person annually, about 10% of what the US spends per person on medical care expenditures.
When faced with a disbursed population, it would be ideal for Public Health to leverage digital tools for health promotion, education, and two-way communication. However, Kern County’s internet access and computer ownership gap is vast.
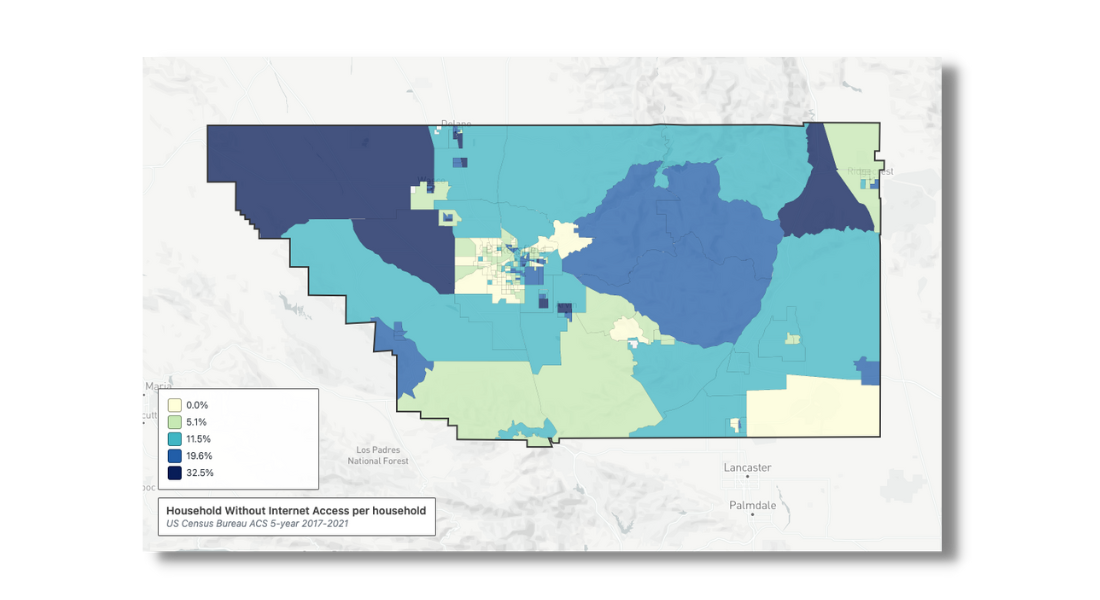
The map above shows the proportion of residents within a census tract who lack internet access. Darker blue areas have fewer internet-connected households, adjusted for population. Like in many counties across the country, rurality predicts internet access. For instance, taking the census tract in the furthest upper-left corner, a deeper dive into the census data reveals that nearly 3,000 people live across a large swath of the county. 94% of residents there identify as Hispanic, and the median income is $42,000 annually. Over half of the residents lack internet in their homes.
Compare this with a tract roughly 30 minutes away, closer to Bakersfield, on the city’s western outskirts. The same number of people reside in this tract, but 99% have internet in their homes. Only 50% identify as Hispanic; the median income is nearly three times greater ($117,000) than the more rural tract.

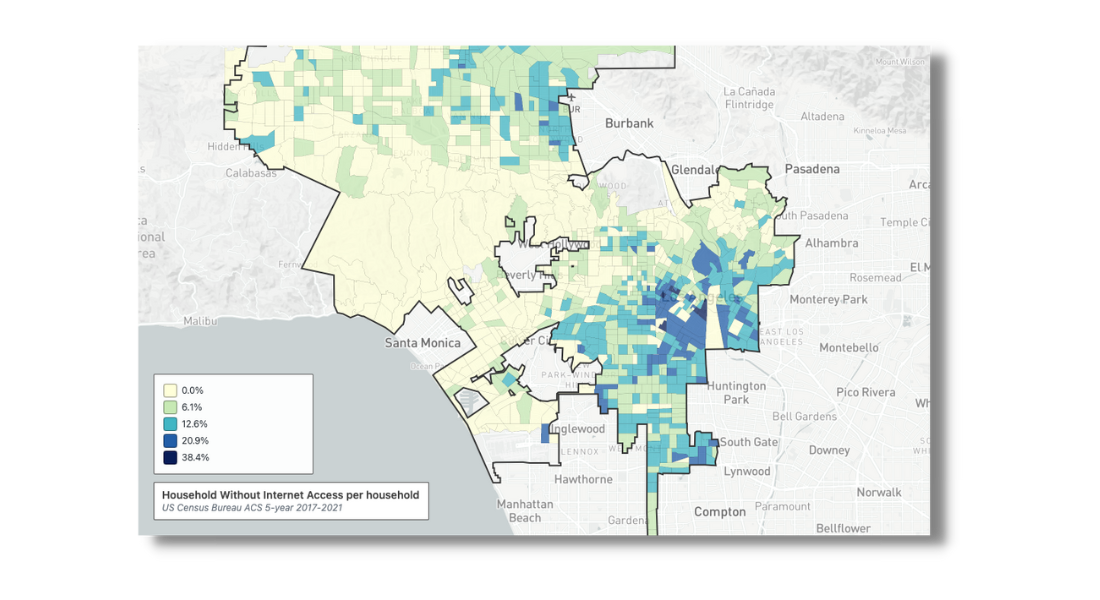
Rurality isn’t the whole story. Even within dense urban centers across the US, race, ethnicity, age, and education level all predict internet access and computer ownership. For example, just 90 minutes from Bakersfield, Los Angeles — one of the country’s most densely populated cities — also experiences a sharp digital divide.
Public Health is forced to operate in an environment that is not conducive to equitable health outcomes. Imagine unveiling a fantastic new Public Health resource website, only to find out that in our rural Kern County example tract, 1500 people might never see it. Now scale that to the entire country, and we’re potentially leaving 14 million people in the dark.
We’ve all learned a ton from the monumental task of testing for and treating COVID-19. Digital tools for population health will look different than tools for clinical care. To protect population health, we must create an infrastructure that combines low-tech and high-tech solutions and design these tools for real humans. Here are just a couple of inspiring examples from our partners who show us that, while the challenge of navigating the digital divide is real, it isn’t insurmountable.
Sometimes the newest approaches can pull from the oldest technology
COVID-19 antiviral telehealth and treatment programs sponsored by state health departments nationwide provide a blueprint for other infectious disease management. With our customers, Color has designed a simple, low-tech alternative to get COVID-19 antiviral treatment to those who need it the most. At Color, we believe that sometimes the most innovative way of bringing health care to everyday places is to rely on everyday resources. So in the case of antivirals, we took it back to basics.
The Color COVID-19 treatment platform allows patients diagnosed with or exposed to COVID-19 to request a virtual visit with a licensed clinician entirely via a phone hotline to evaluate whether antiviral treatment is appropriate. The intake is completed with the patient’s verbal consent, allowing patients without internet-enabled devices to request a visit. If the patient is eligible for the program, the clinician will conduct the virtual visit over the phone. If the clinician decides that treatment is appropriate, the patient can choose home delivery or pickup from a preferred pharmacy. Our platform supports 16 different languages, ensuring that we’re able to communicate clearly with in our most diverse communities. As of March of 2023, in some states we operate, we’re even able to offer care for dependents who are 12 and older. As one resident in Washington State told us:
“I signed in last night and within 90 minutes had met virtually with a provider and had the medication in hand. Much better response than my local clinics who wanted me to wait over 60 hours for the next virtual visit.”
Public Health can (and should) happen anywhere
If we want to bridge the digital divide, we need to go where the people are, using the tech they do have. Internet access via mobile phones is at an all-time high, and 85% of Americans own a smartphone. Mobile-optimized tools can be a lifeline for households without a computer, so low-fidelity outreach solutions are crucial to success.
Knowing cell phones are nearly ubiquitous, Color partnered with Allegheny County, PA to innovate how Public Health screens, tests, and treats sexually transmitted infections (STIs). Created for youth ages 18-25, this initiative combined deliberately placed social media ads on popular sites such as Instagram and Grindr with mailed STI test kits designed for a private, stigma-free approach to care. This program is an ideal example of Public Health at its best: culturally appropriate outreach coupled with simple tools and a robust continuum of care. We’ve seen similar success in our approach to cervical cancer prevention and are optimistic that, together with the fantastic governmental partners we are honored to work with, there isn’t anything we can’t accomplish. The future of Public Health is bright.
Until we exist in a country with internet broadband infrastructure covering all people, the digital divide is a barrier to health equity. In light of this, we will continue to invest in Public Health infrastructure tools that work with what people have and find them wherever they are.
If you want to learn more about how Color brings extraordinary care to everyday places, reach out to us. One of our solution design experts will be in touch shortly.